Evaluation and Management of Antenatal Hydronephrosis
Article information
Abstract
Antenatal hydronephrosis (ANH) is one of the most common abnormal findings detected on prenatal ultrasound (US), and it has been reported in 1-5% of all pregnancies. The likelihood of significant postnatal pathologic abnormality in the urinary tract correlates with the degree of anterior-posterior diameter (APD) according to the gestational age. Detection of urologic anomalies prenatally permits fetal interventions that avoid complications in rare cases of bladder outlet obstruction with oligohydramnios even though their final benefits still remain controversial. There is no clear consensus on the extent and mode of postnatal imaging after a diagnosis of ANH. US is the mainstay of the postnatal evaluation and helps guide further testing with voiding cystourethrography (VCUG) and diuretic renography. Although most algorithms continue to recommend generous VCUG for identification of lower urinary tract anomalies, VCUG may be safely reserved for high grade ANH cases or any grade of ANH with dilated distal ureter without increasing the risk of urinary tract infection (UTI). There are conflicting studies about efficacy of postnatal prophylactic antibiotics. It still seems reasonable to consider use of a prophylactic antibiotic to prevent infant UTIs in high-risk populations, such as females and uncircumcised males with high grades of hydronephrosis, hydroureteronephrosis, or vesicouretral reflux.
Introduction
Increasing use of ultrasound (US) has allowed an appreciation of the true incidence of urological abnormalities, the most common of which is hydronephrosis (HN). Antenatal hydronephrosis (ANH) is the most common urological abnormality detected on prenatal US, and it has been reported in 1-5% of all pregnancies. There are various urological conditions from transient dilation of the renal collecting system to severe obstructive uropathy requiring surgical interventions. The purpose of evaluating children with ANH is to distinguish clinically significant urological conditions from transient HN with little clinical significance. However, the diagnostic criteria for identification of children at risk for renal damage remain a subject of debate and the clinical guideline of ANH has yet to be clearly established. This article reviews the current literature regarding the perinatal evaluation and management of ANH.
Definition of ANH
1. APD (anterior-posterior diameter)
APD of the renal pelvis is the most commonly studied indicator for assessing ANH and a sentinel of potential diseases, however, it does not identify specific underlying pathology [1-3]. Potential factors affecting APD are gestational age, hydration status of the mother, and the degree of bladder distention [4-9]. Since the dimensions of the renal pelvis may normally increase with gestational age, most investigators have adjusted threshold APD values according to the gestational age (Table 1) [10]. Limitations of APD as a tool of ANH are as follows, (1) it is single measurement of collecting system, (2) there would be the inter- and intra-observer reliability, and (3) APD does not consider calyceal dilation or renal parenchymal thinning that may indicate more severe obstruction.
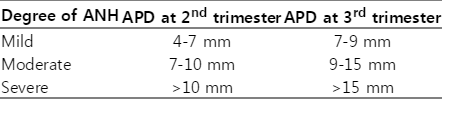
Degree of Antenatal Hydronephrosis (ANH) according to Renal Pelvic Anterior-posterior Diameter (APD) Adjusted for Gestational Age
2. SFU grading (Table 2 [11])

SFU Grading of Infant Hydronephrosis
At Grade 0 there is no HN, so the central renal echo complex is closely apposed. At Grade 1 the renal pelvis only is visualized with slight separation of the central renal echo complex, At Grade 2 the renal pelvis is further dilated and a single or a few but not all calices are identified in addition to the renal pelvis. Grade 3 HN requires that the renal pelvis is dilated and there are fluid filled calices throughout the kidney, but the renal parenchyma is of normal thickness. Grade 4 HN may have a similar appearance of the calices as Grade 3 but, when compared with the normal side, the involved kidney has parenchymal thinning over the calices.
3. Significant US findings associated with ANH
Loss of cortico-medullary differentiation, increased parenchymal echogenicity and the presence of renal cysts are associated with the loss of functional renal parenchyma [12-14]. Perinephric urinoma can be seen in severe urinary obstruction. ANH is more likely to be associated with postnatal pathology when it is accompanied with parenchymal thinning, calyceal dilatation, ureteral dilatation, chromosomal anomalies, and multiple system malformations. Oligohydramnios (OHA) appears to be one of the most important predictive factors for postnatal pathology. Multivariate analyses have identified OHA and megacystis to be predictive of urethral obstruction, and OHA to be predictive of chronic renal failure or death [15, 16]. Also, another multivariate analysis in children with posterior urethral valve (PUV) has identified OHA to be predictive of chronic renal failure [17].
Underlying pathology of ANH
The most common cause of ANH is transient HN which resolves as time goes. Ureteropelvic junction (UPJ) obstruction is the most common underlying pathology of ANH and its incidence ranges from 10 to 30%[10]. Level of ureteral obstruction can be as low as ureterovesical junction (UVJ). UVJ obstruction usually, not always, causes dilation of the entire ureter, which is called as hydroureter. Incidence of vesicoureteral reflux (VUR) as a cause of ANH has been reported from 10 to 20%. Multicystic dysplastic kidney as well as ureterocele-ectopic ureter-duplex system are other causes of ANH. Relatively rare causes of ANH are PUV, prune belly syndrome, mid-ureteric stricture, and megalourethra.
Antenatal radiological evaluation and intervention for ANH
It is generally recommended that the prenatal identification of HN (APD >4 mm in the 2nd, or >7 mm in the 3rd trimester) requires further follow up. The presence of findings suspicious of PUV, such as OHA, dilated bladder, bilateral hydroureteronephrosis (HUN), warrants monitoring throughout pregnancy, and any co-morbid fetal abnormality should also be investigated. Depending on the severity of OHA, fetal imaging may be needed every 4 weeks. However, in the presence of increasing OHA, fetal intervention such as vesicoamniotic (VA) shunting may be offered. The ideal time period to offer prenatal intervention for suspected bladder outlet obstruction appears to be the mid-second trimester. This will allow for the return of amniotic fluid, in an effort to promote fetal lung development. A gross predictor of renal function may be obtained by performing a fetal bladder tap and analysis of fetal urine biochemistries and electrolytes [18]. Due to the first pass of urine into the bladder, it is recommended to make all decisions based on a repeat fetal bladder tap within 48 hours of the initial bladder decompression. If favorable urine electrolytes are obtained, fetal intervention may be offered as an option. According to a recent randomized trial done by Morris et al. [19], survival seemed to be higher in the fetuses receiving VA shunting. On the other hand, there also is another recent study supporting that prenatal interventions do not improve prognosis of babies with OHA associated renal and urinary tract anomalies [20].
Postnatal radiological evaluation
The initial postnatal evaluation of ANH depends in part on the degree of HN seen during fetal evaluation. Currently, no study is considered a gold standard for the evaluation of renal obstructive disorders and complete assessment typically involves a series of studies including US and diuretic renal scintigraphy (DRS). Even though there is no consensus on the optimal APD threshold for determining the need for postnatal follow up, according to a recent study, isolated HN with APD more than 16mm on US performed at 7-30 days after birth warrants further investigation including VCUG [21]. VCUG is frequently performed in conjunction with renal studies to rule out VUR as the cause of HN. It should be kept in mind that VUR may coexist with UPJ obstruction in as many as 10% of children [22]. Currently, there is no clear evidence to support or to avoid postnatal imaging for VUR. Neither the grade of the HN nor gender is a predictive factor for VUR in children with ANH. The overall incidence of VUR is up to 30% in children with ANH, including those with resolved HN [3, 23]. It remains unproven whether the identification and treatment of children with VUR confers any clinical benefit because most patients with VUR and low grade HN can be followed without surgical intervention. According to SFU 2010 recommendations for VCUG timing after renal US, neonates with moderate to severe bilateral ANH need to get VCUG within a week after birth. Any episode of moderate or severe HN on two US tests (pre- and postnatal US) warrants VCUG within 4 weeks [10]. However, newer SFU recommendations published in 2013 proposed APD 9 mm or greater and SFU grade 3 or greater at third trimester as an independent predictors of postnatal intervention while supporting that most patients with VUR and low grade HN can be followed without surgical intervention. Patients with a SFU grade of 4 progressed to surgical intervention at a faster rate than those with a grade of 3 [24].
Biomarkers and HN
Advances in the field of biomarkers have opened the possibility to predict the risk of obstruction and renal functional impairment in infants with ANH. These potential biomarkers include transforming growth factor beta 1 (TGF-β1), urinary monocyte chemotactic protein-1 (UMCP1), urinary neutrophil gelatinase-associated lipocalin (NGAL), and beta-2- microglobulin (β2-M). TGF-β1 is known to be associated with renal dysplasia, acquired renal damage, and obstruction [25, 26]. However, this marker has not been shown to be associated with HN grade [27]. UMCP-1 has also been evaluated as a potential marker of UPJ obstruction. A recent case-control study showed that UMCP-1 is elevated in cases of urinary obstruction and positively correlates with T1/2 radiotracer clearance and impaired split renal function on DRS. However, UMCP- 1 may be a nonspecific measure of renal injury rather than unique to obstructive nephropathy, as with TGF-β1 [28, 29]. Both urinary NGAL and β2-M have been studied as markers of preoperative obstruction and postoperative success. Madsen et al. found that both NGAL and β2-M increased in patients with evidence of obstruction at the time of pyeloplasty and that these levels decreased to levels similar to healthy controls after surgical correction [30]. Cost et al. also found that NGAL levels were significantly higher in children with UPJ obstruction and returned to normal after surgical repair. Interestingly they found that NGAL levels were inversely correlated with split renal function, suggesting that NGAL may serve as a marker for both obstruction and renal impairment [31].
Urinary tract infection (UTI) and ANH
The rationale for antibiotic prophylaxis in children with a history of ANH includes prevention of UTIs, as infants with HN are at increased risk [32]. The risk of UTI increases with increasing grade of HN [33]. Rates appear to be as high as 40% in children with SFU grade 4 HN [34], with another study estimating the cumulative incidence of UTI as 39%, 18% and 11% at 36 months of age for severe, moderate and mild renal pelvic dilation, respectively [33]. Several studies report a higher rate in girls compared to boys [32, 33]. Children with HN and obstructive drainage patterns on DRS are at increased risk compared to those without obstructive patterns [34, 35]. An increased risk is also associated with hydroureteronephrosis (HUN) even without VUR or without an obstructive pattern on DRS [35, 36]. These observations suggest that increased stasis and easier access to a urinary reservoir (such as in the case of hydroureter) increase the chance of developing a UTI.
The efficacy of antibiotic prophylaxis
High rates of UTI have been noted despite prophylactic antibiotics in children with HN [33]. Similarly there was a report that there was no statistical difference in the incidence of UTI in children with ANH on or off prophylactic antibiotics [37]. In contrast, Estrada et al. [38] observed that in children with a history of ANH with persistent grade II HN secondary to VUR, the use of prophylactic antibiotics significantly reduced the risk of febrile UTIs. According to a recent systemic review [39], offering continuous antibiotic prophylaxis (CAP) to 7 infants who have high-grade HN would prevent 1 UTI, suggesting value in this subgroup of patients. While the literature has both supportive and contradictory evidence, the growing trend not to place children with ANH on CAP has created varied clinical practice based on anecdotal individual case characteristics. However, consensus on what constitutes a risk factor for UTI warranting CAP in this population should be determined. SFU 2010 recommendations advocated the use of CAP to prevent infant UTIs in high-risk populations, such as with higher grades of HN, HUN, VUR, or obstructive drainage patterns [10]. Herz et al. retrospectively studied predisposing risk factors to febrile UTI by comparing 405 children with and without CAP. The presence of ureteral dilation, high grade VUR, and UVJ obstruction were independent risk factors for development of UTI in children with ANH [40]. Braga et al. prospectively investigated the impact of risk factors for febrile UTI in 334 infants with postnatally confirmed ANH, and they identified female gender, uncircumcised males, HUN, VUR and lack of CAP as risk factors for febrile UTI. Subgroup analysis excluding VUR showed that high grade ANH was also a significant risk factor [41].
Conclusions
ANH, one of the most common abnormal finding on antenatal US, continues to increase as the standard of care includes 2nd trimester US. While rare cases may be associated with pathology such as PUVs that require perinatal interventions, it is both safe and reasonable, in most cases, to wait for spontaneous improvement with the intensity of follow-up depending on the grade of ANH. US is the mainstay of the postnatal evaluation and VCUG may be safely reserved for high grade ANH or dilated distal ureter. New urinary biomarkers may offer promising potential for more accurate risk stratification in the near future. While there have been conflicting studies about efficacy of postnatal CAP, it seems reasonable to consider use of CAP in children with high risk of UTI.
Notes
Conflict of interest
None of the contributing authors have any conflict of interest, including specific financial interests or relationships and affiliations relevant to the subject matter or materials discussed in the manuscript.




