Pediatric Acute Kidney Injury: Focusing on Diagnosis and Management
Article information

Abstract
Acute kidney injury (AKI) is common in critically ill children, and is associated with increased mortality and long-term renal sequelae. The definition of pediatric AKI was standardized based on elevation in serum creatinine levels or decrease in urine output; accordingly, epidemiological studies have ensued. Although new biomarkers appear to detect AKI earlier and predict prognosis more accurately than traditional markers, they are not frequently used in clinical setting. There is no validated pharmacological intervention for AKI, so prevention and early detection are the mainstays of treatment. For high risk or early stage AKI patients, optimization of volume status and blood pressure, avoidance of nephrotoxins, and sufficient nutritional support are necessary, and have been demonstrated to be effective in preventing the occurrence of AKI and improving prognosis. Nevertheless, renal replacement therapy is needed when conservative care fails.
Introduction
Acute kidney injury (AKI) is characterized by an abrupt deterioration of kidney function, and is common in critically ill children and adults. It occurs in approximately 30% of pediatric intensive care unit (PICU) [1]. Pediatric AKI has been associated with higher morbidity and mortality after adjustment for other risk factors [1], and is a risk factor for hypertension and chronic kidney disease (CKD) in the long term [2,3]. Recently, many studies have been conducted in the field of pediatric AKI following adult studies and have prompted new interest. This review summarizes pediatric AKI, with a focus on diagnosis and management.
Definition of AKI
In 2012, the Kidney Disease: Improving Global Outcomes (KDIGO) criteria were established, and provided a standardized definition of AKI in children and adults [4]. It was characterized by elevation in serum creatinine levels and/or decrease in urine output, based on the previously well-known, Risk, Injury, Failure; Loss, End-Stage Renal Disease (RIFLE) and Acute Kidney Injury Network (AKIN) criteria (Table 1) [4]. The severity of AKI is staged according to the amplitude of serum creatinine elevation form baseline value or the duration of compromised urine output.
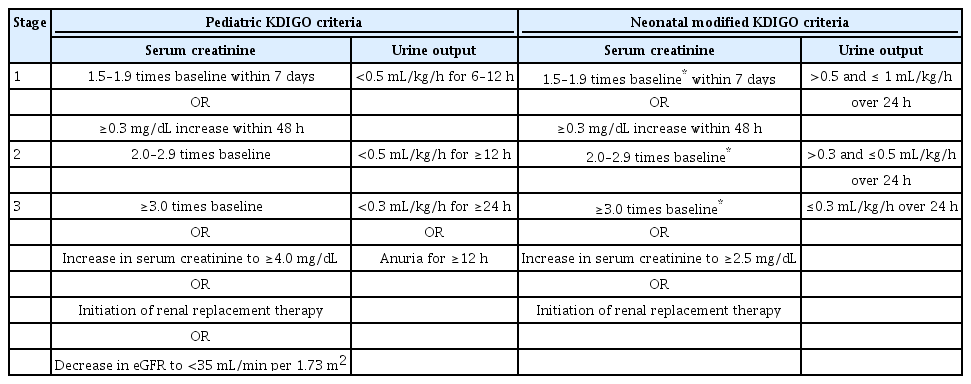
Definitions and Staging of Kidney Disease: Improving Global Outcomes (KDIGO) and Neonatal Modified KDIGO Criteria for Acute Kidney Injury
Physicians sometimes, however, experience difficulty in diagnosing and staging AKI using the KDIGO definition. Many patients exhibit elevated serum creatinine levels without previous measurement. It is not integrated to set baseline value without available measurement data within 48 h, as specified by the KDIGO criteria. Some have used the lowest serum creatinine level measured before or after AKI as a baseline value. Others propose that the baseline serum creatinine level can calculate backward using an estimated glomerular filtration rate (eGFR) of 100–120mL/min/1.73 m2, assuming that previous kidney function was norma [5].
For neonates, the neonatal modified KDIGO definition was used in a recent large cohort (Table 1) [6,7]. Although it is based on a modification of the KDIGO definition, it is different with urinary output checked in 24 h blocks. Moreover, the baseline value is the lowest previous serum creatinine level because serum creatinine, which reflects maternal creatinine in the first few days, declines physiologically within weeks of life at a rate that varies with gestational age [8,9].
AKI biomarkers
Serum creatinine is currently widely used as a biomarker for AKI; however, it has some limitations. It is insensitive to small changes in GFR, and is not a real-time indicator. It may not change until up to 50% of kidney function is lost [10], and rise up to 72 h after an insult. Furthermore, its concentration is affected by age, sex, muscle mass, and volume status [11]. For two decades, many researchers have been searching new biomarkers that are rapid, sensitive, specific, inexpensive, noninvasive, and unaffected by clinical factors [12]. Cystatin C, neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1, N-acetyl-β-D-glucosaminidase, interleukin-18, liver-type fatty acidbinding protein, cycle arrest markers, and BPI containing family A member 2 have been evaluated. These appear to detect AKI earlier and predict prognosis more accurately than serum creatinine levels [12].
Serum cystatin C is produced by all nucleated cells and, is therefore, unaffected by clinical factors [13]. Its level rises earlier (12–24 h after insult) than that of serum creatinine [14]. In studies involving specific pediatric populations (children who underwent cardiac surgery, treated with aminoglycoside or contrast agent, and preterm infants with respiratory distress syndrome), it predicted AKI earlier than serum creatinine level, predicted persistent AKI, and showed greater sensitivity and specificity [14-17]. Its disadvantage is that it is affected by high-dose corticosteroids, inflammation, and systemic diseases [18]. NGAL, a proximal tubular protein, is the most rapid predictive biomarker, and is elevated <2 h after insult [19]. Studies investigated NGAL in pediatrics have mainly involved patient undergoing cardiac surgery, and have reported that elevation of urinary NGAL was associated with poor prognosis [20,21]. Urinary NGAL increases during urinary tract infection, sepsis, and CKD regardless of AKI [22]. A combination of two cell-cycle arrest markers urinary tissue inhibitor of metalloproteinase-2 and insulin-like growth factor-binding protein 7 demonstrated high sensitivity (90%) and low specificity (49%) in critically ill adults [23], and was approved by the United States Food and Drug Administration for use in adults. A few studies have shown that it has good diagnostic performance in pediatric, and neonatal AKI [24,25].
Despite the excellent performance of new biomarkers, they are not frequently used in clinical setting due to several concerns. First, they were validated for specific etiologies of AKI, such as pediatric patients undergoing cardiac surgery, and their efficacy cannot be reproduced in AKIs of different etiologies [12]. Moreover, they are also elevated in other clinical conditions, such as inflammation [12]. Large prospective studies investigating and validating the clinical utility of these biomarkers, therefore, is warranted.
Incidence
Two large, multinational epidemiological studies have been published in the pediatric and neonatal areas [1,7]. The Assessment of Worldwide Acute Kidney Injury, Renal Angina, and Epidemiology (AWARE) study described the epidemiology of AKI in 4,683 pediatric patients (age range 3 months to 25 years) who were admitted to the PICU [1]. It reported that AKI developed in 26.9% of patients and KDIGO stage 2 or 3 AKI in 11.6% within 7 days of PICU admission [1]. The Assessment of Worldwide Acute Kidney injury Epidemiology in Neonates (AWAKEN) study described neonatal AKI in the neonatal ICU, and reported a prevalence similar to that of the AWARE study. The incidence of AKI was 29.9%, with 13.9% reaching AKI stage 1, 7.1% reaching AKI stage 2, and 8.9% reaching AKI stage 3 [7]. The incidence outside the ICU varies across medical centers. To our knowledge, there have been no large-scale studies investigating AKI in non-critically ill children in Korea.
Outcomes
In the pediatric literature, AKI is consistently associated with poor outcomes, similar to adults. Many studies have demonstrated that AKI is an independent risk factor for prolonged stay in the PICU, longer duration of mechanical ventilation, and increased mortality among critically ill children [1,26,27]. In addition, several observational studies have reported a high prevalence of CKD, hypertension, and proteinuria among AKI survivors [28-30]. Neonatal AKI is also a risk factor for mortality [7]. There have been no sufficiently large follow-up studies evaluating the relationship between neonatal AKI and long-term renal insufficiency. However, small observational studies have reported a high prevalence of CKD, and proteinuria in survivors of neonatal AKI [29,31].
Management
1. Risk factors and prevention
There are no effective medications for established AKI. Therefore, prevention and early detection are the mainstays of management. Monitoring high-risk patients and reducing additional risk factors can prevent the occurrence of AKI and improve outcomes. Prematurity, and chronic diseases such as CKD render the host susceptible to AKI, and events such as volume depletion, exposure to nephrotoxins, sepsis, major surgery, and critical illness lead to AKI [4]. The renal angina index was proposed to predict AKI in critically ill children on the basis of subtle kidney injury (changes in estimated creatinine clearance or fluid overload) and patient risk factors (ICU admission, stem cell transplantation, ventilation and inotropy) [32].
Despite its importance, physicians often do not devote attention to the accumulation of risk factors and early decline of kidney function as they perform or attend to other important aspects of care [33]. Recently, a system using electronic health records was implemented and helped physicians detect AKI early and mitigate the influence of risk factors [34]. The system electronically flags high-risk patients to the medical team in near real-time. As such, the medical team does not miss high-risk patients and monitors them carefully. It has been shown to improve the rate of recovery from AKI [35]. In the pediatric literature, this system was developed to screen children who experienced multiple nephrotoxin exposures, which prompted clinicians to monitor more closely for the development of AKI. It demonstrated a positive effect in decreasing exposure to multiple nephrotoxins and, finally, AKI events [36].
2. Supportive care
Supportive care comprises optimization of volume status, blood pressure, avoidance of nephrotoxic agents, and nutritional support. It is important to maintain adequate renal perfusion through fluid and hemodynamic management [37]. Volume status should be optimal (i.e., not excessive, not insufficient). The medical history and symptoms are important to evaluate volume status. Body weight, fluid intake, urine and stool output, and vital signs should be monitored daily, and lung sound and lower extremity edema should be checked [38,39]. Serum chemistries and chest X-ray are also useful. Although volume depletion is a well-known risk factor, volume overload is associated with poor prognosis [40]. Fluid accumulation in the acute phase, which is common in the PICU, is associated with high mortality in critically ill patients [40,41]. The pediatric literature suggests that 10–20% fluid overload is a critical threshold at which outcomes are negatively impacted [41,42]. Administration of optimal fluid amount is crucial. Patients with a normal intravascular volume should initially be limited to insensible losses (400 mL/m2/d) plus an amount of fluid equal to the urine output and extrarenal loss [38]. Noticeable hypervolemic patients require further fluid restriction, omitting the replacement of insensible fluid losses, urine output, and extrarenal losses while considering adequate nutritional support [38]. Diuretics therapy, especially loop diuretics, should be considered for hypervolemic patients. The pediatric literature shows that clinicians should consider initiating renal replacement therapy (RRT) at a fluid overload of >20%, while a fluid overload 10–20 % requires further evaluation [42].
The proper type of fluid should be administered to prevent volume depletion. Crystalloids are the preferred solutions because data supporting the routine use of colloids for volume resuscitation are lacking [43]. Colloid solution was not superior to crystalloid in terms of the prevention of AKI in children who underwent cardiac surgery [44]. Among crystalloids, some studies have reported that a balanced solution, such as Ringer’s lactate solution, is superior to normal saline [45]. Balanced solutions are defined as intravenous fluids having an electrolyte composition close to that of plasma. They have low chloride content of about 100–110 mmol/L, which is the most altered in normal saline as compared to plasma [46,47]. Normal saline, which is hyperchloremic, can cause hyperchloremic metabolic acidosis, contributing to impaired recovery and poor clinical outcomes [48]. Three recent large prospective studies have reported conflicting results [49-51]; as such, debate regarding which solution is best among crystalloids continues.
Maintaining optimal blood pressure is crucial, although there is no currently definitive target value for pediatric AKI. For patients with hypotension, fluid resuscitation is initially considered if hypotension is due even partially to hypovolemia [18]. Norepinephrine is recommended if hypovolemia is not suspected [52]. High blood pressure in patients with AKI is mostly due to volume overload or disturbed renin-angiotensin axis [22]. Diuretics are attempted first unless patients exhibit signs of intravascular depletion [22].
Nephrotoxin exposure is one of the most common causes of AKI in hospitalized children [53]. Critically ill patients who are at high risk for AKI have the opportunity to be administered nephrotoxic mediations. Amphotericin, aminoglycoside, vancomycin, nonsteroidal anti-inflammatory drugs, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, calcineurin inhibitors, cisplatin, and methotrexate are well-known nephrotoxins [18]. Clinicians must balance the therapeutic benefits versus the risk for nephrotoxicity. If the use of nephrotoxic medications is inevitable, their dosage or dosing interval should be adjusted and monitored to reduce renal toxicity. Drug levels should be measured, if possible, and adjusted accordingly. If not possible, medications should be adjusted based on eGFR. Be aware that eGFR does not account for real-time renal function in AKI [22]. Contrast agent used for computed tomography and angiography are nephrotoxic. Contrastinduced AKI is common in children [54], and risk depends on the contrast agent dosage and type. Angiography requires more attention because it requires more contrast agent than computed tomography. High-osmolality contrast agent carries a higher risk for AKI, but have been replaced by low-osmolality contrast agents, which have a lower risk [55]. Nevertheless, patients with a GFR <60 mL/min/1.73m2 or at high risk for AKI should be prepared before exposure [22]. The key preventive measure is hydration. An isotonic crystalloid solution at 1 mL/kg/h should be administered intravenously for 12 hours before and after the procedure [18]. If contrast agent should be administered urgently, 3 mL/kg/h 1 h before and 6–9 mL/kg over 4–6 h after the procedure should be administered [18]. In addition, nephrotoxins should be discontinued for >24 h before the procedure [18]. The use of N-Acetylcysteine (NAC) will be discussed below.
Nutritional support is important for improving outcomes in children with AKI. For critically ill children with AKI, nutritional requirements should be individualized and assessed frequently [56]. In general, 120–130% of basal calories needs, and 2–3 g/kg/day of protein should be provided [56], and hyperglycemia should be avoided [57].
3. Pharmacological treatment
Many researchers have investigated candidate medications to prevent and treat AKI. Anti-inflammatory, antioxidative and antiapoptotic interventions are representative examples; however, their yield remains insignificant. Although a few medications have demonstrated effectiveness in certain situations, most have yielded negative or conflicting results. Medications advocated in the past were not proven to be effective. The KDIGO guideline recommend NAC to prevent contrast-induced AKI in high-risk patients [4]. However, two large, well-designed studies reported no benefit of NAC in reducing the incidence of contrast-induced AKI [58,59]. Diuretics are not recommended for the prevention of AKI because their use does not alter outcomes in those with established AKI [60]. Diuretics should be used only to control fluid overload. Low-dose dopamine and fenoldopam did not have a positive effect on protection against AKI [61,62]. Perioperative statins did not reduce the incidence of AKI among patients undergoing cardiac surgery [63]. Even now, candidate medicines, such as recombinant alkaline phosphate, costimulatory molecule CD28 receptor antagonist, p53 small interfering RNAs, and mesenchymal stem cells, are under consideration [18]. To establish the basis for routine clinical use of new medications, additional multicenter, high-quality trials are warranted.
4. RRT
RRT is required when conservative care fails. Indications for RRT include fluid overload (severe hypertension or pulmonary edema), severe hyperkalemia, metabolic acidosis, and severe uremia [64]. The optimal timing of RRT initiation remains controversial. A recent meta-analysis of randomized controlled trials revealed that early initiation of RRT does not reduce mortality when compared with standard or late initiation in adults [65]. Although one investigation involving pediatric patients demonstrated that early initiation improved mortality in cardiac surgery patients [66], it was small and retrospective in design; thus, more studies are needed. RRT modalities for AKI have begun with peritoneal dialysis and hemodialysis, and are now expanding to continuous renal replacement therapy (CRRT). We believe that all of these modalities represent viable management options in pediatric AKI [67]. There is no definite evidence that one dialysis modality is superior to another in terms of outcomes in AKI [68,69]. The modality should be determined according to the patient characteristics, institutional resources, and expertise [69]. Each modality has advantages and disadvantages. Peritoneal dialysis can be used in small children such as preterm infants, but removes fluid and waste slowly and unpredictably [67]. Hemodialysis removes toxins rapidly, but is dangerous for small children and hemodynamically unstable patients [67]; additionally, it requires expertise. Currently, CRRT becomes the preferred modality in developed countries as improvement of equipment [69]. CRRT facilitates hemodynamic stability and make it possible to use them in small children, such as neonates. New devices, such as the Cardio-Renal Pediatric Dialysis Emergency Machine, and Newcastle Infant Dialysis and Ultrafiltration System, have provided promising results for the treatment of neonates requiring RRT [70,71]. However, the device should be operated in the PICU, so that children must endure anxiety about being separated from their parents during treatment.
Conclusion
AKI has attracted attention because of its high prevalence and association with poor outcomes. Many studies have been conducted to identify new biomarkers and effective pharmacological interventions, and significant improvements have been achieved. Unfortunately, however, not many have been applied in actual clinical practice. Considering the gap between research achievements in adults and children, pediatric nephrologists have much to contribute to developments in understanding and treating AKI.
Notes
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Conflict of interest
No potential conflict of interest relevant to this article was reported.