Calcified Macroplastique Substance: A Rare Cause of Recurrent Gross Hematuria after Endoscopic Injection
Article information
Abstract
Endoscopic subureteral injection for treatment of vesicoureteral reflux (VUR) is known to be safe and efficient due to its minimal invasive nature. Being non-migratory, non-antigenic, and biocompatible, Macroplastique (Polydimethylsiloxane) is likely to be stable over time. A 5-year-old boy with a past history of subureteral administration of Macroplastique for unilateral Grade V VUR 4 years ago presented with recurrent gross and microscopic hematuria, along with suprapubic pain. On computed tomography (CT) abdomen, calcified material, suspected to be a stone, was visualized in the bladder. On diagnostic cystoscopy, calcification was seen around the orifice site where Macroplastique injection had been performed. We removed the calcific material by Holmium laser. Endoscopic subureteric implantation has several advantages, but nevertheless, vigilance is needed to detect long-term complications, especially in patients with gross or microscopic hematuria.
Introduction
Vesicoureteral reflux (VUR) is present in about 1% of normal healthy children and in 30–50% of children with symptomatic urinary tract infections (UTIs) [1]. The most common presenting symptom of VUR is pyelonephritis, which can lead to renal injury and subsequent renal impairment or end-stage renal disease [2]. Children with VUR may be managed either medically or surgically. The rationale for medical management is prevention of UTI using daily antibiotic prophylaxis, regular timed voiding and, in some cases, anticholinergic medication. The surgical management of VUR consists of repair of the ureterovesical junction (UVJ) abnormality [3]. In recent years, endoscopic subureteral transurethral injection (STING) has become the first-line therapy for children with VUR owing to its high success rate and minimum complications [4]. The substance used for endoscopic injection should be nontoxic, biocompatible, non-migratory, and non-antigenic, causing minimal local inflammation. Macroplastique is one of the most popular bulking agents and has wide application in the medical field, especially in endoscopic management of VUR [5]. We report a case of gross hematuria caused by calcified Macroplastique substance injected to initially treat unilateral VUR.
Case report
A 5-year-old boy presented to our pediatric emergency department with intermittent gross hematuria and suprapubic pain since several months. He was treated with antibiotics for suspected cystitis, whenever he had such symptoms in the past and symptoms were disappeared in several days. He suffered from recurrent febrile UTIs since 4 months of age, and was diagnosed with unilateral grade V VUR and the febrile UTIs were not responsive to prophylactic antibiotics, hence Macroplastique injection was performed at 9 months of age (Fig. 1).
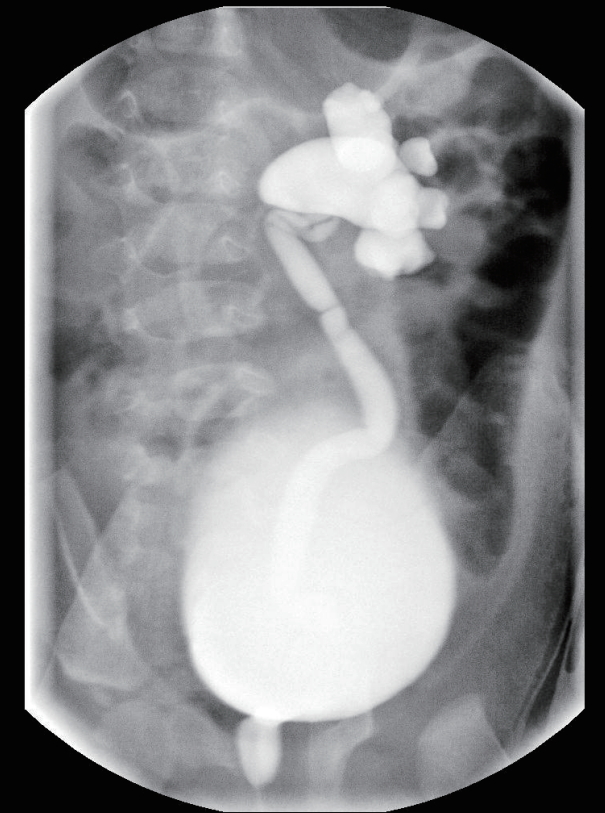
Voiding cystourethrography shows grade V reflux before intraureteral Macroplastique injection therapy.
Follow-up VCUG performed 3 months after injection showed a resolution of VUR. After 2 years from Macroplastique injection, gross hematuria appeared first time. Also, two times microscopic hematuria and three times gross hematuria broke out. His mother gave a history of transparent powdery material in his urine frequently, after Macroplastique injection. Whenever hematuria presented, we checked urine calcium/creatinine ratio and the results were always within age specific reference ranges. Also his 24 hours urine calcium was 19.76 mg (1.31 mg/kg). On examination, he was afebrile with stable vital signs. Initial urinalysis showed isomorphic hematuria and mild proteinuria.We performed CT abdomen, which demonstrated two 0.7 cm hyperdense lesions in the left posterior aspect of the bladder and suspected stones at the UVJ or in the bladder (Fig. 2). Ultrasonography (US) showed previous mild pelviectasia of the left kidney (0.3 cm) and two hyperechoic foci with posterior acoustic shadowing, in the left posterior aspect of the bladder. However, the lesion did not move with position changes. Therefore, to find out the exact problem, considering a past medical history of Macroplastique injection, we decided to perform a diagnostic cystoscopy.
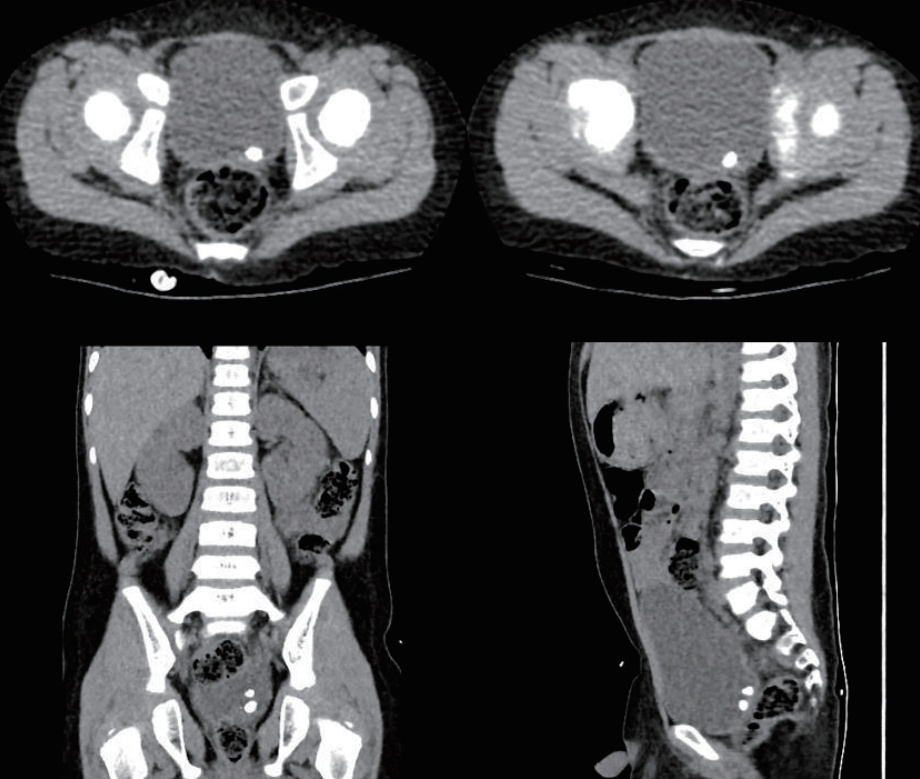
Computed tomography image shows 0.7cm sized hyperdense lesions in bladder.
On cystoscopy, calcifications were seen, leading to mucosal erosions around the orifice where Macroplastique injection had been injected previously. The calcifications on the mucosal area causing mucosal erosion were successfully removed with the help of laser (Fig. 3). Symptoms of gross hematuria, suprapubic pain, and dysuria were gradually relieved after treatment. We have checked routine urinalysis and US after seven months from cystoscopy. There were no identifiable calcifications in bladder mucosa although we cannot exactly evaluate as follow up CT scan was not done. His symptoms have not recurred till date.
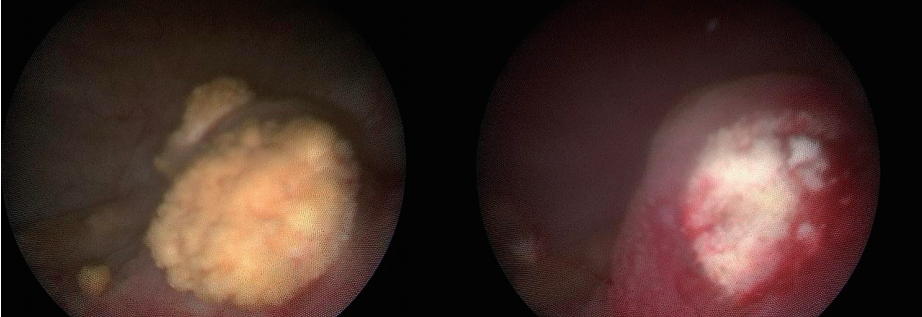
(A) On diagnostic cystoscopy, 0.7cm sized yellowish impacted stones were observed at left posterior aspect of the bladder. (B) Mucosa erosions were observed and stones were removed by Holmium laser.
Discussion
Endoscopic subureteral injection has gained popularity and has evolved as the prime therapeutic alternative to antibiotic prophylaxis and ureteroneocystostomy, since its initial description by Matouschek in 1981, and its first clinical use reported by O’Donnell and Puri in 1984 [6,7]. Intraoperative complications following injection of bulking agent had a remarkably low incidence, and complications were limited to infection and/or bleeding. Postoperative complications were also extremely rare [8]. Several bulking agents with numerous advantages as well as drawbacks have been used to treat reflux, including polytetrafluoroethylene, collagen, autologous injectables, Macroplastique (Uroplasty, Minnetonka, USA), and dextranomer/hyaluronic acid copolymer (Deflux; Oceana Therapeutics, Inc, Edison, USA). Among these agents, Macroplastique is one of the most popular agents and has wide application in the medical field. Macroplastique, made of solid silicone elastomer, a non-biodegradable substance, is reabsorbed and exchanged with a reactive transudate containing fibroblasts, which then facilitate its encapsulation [4]. Since the success rate was dependent on the kind of bulking agent injected, many studies have demonstrated the overall success rate of each material, and no significant difference was observed in cure rates [4,9]. Some previous studies have reported that VUR was better corrected in the Macroplastique group (86.2%) than in Deflux group (71.4%) [5]. Most studies focus on success rates, but postoperative complications after endoscopic therapy of VUR, or procedure-related complications (obstruction, contralateral VUR, voiding anomalies) should be evaluated, to confirm overall safety of the procedure or operation [1]. One study demonstrated several short-term complications after endoscopic injection of Macroplastique. Four patients who had recurrent UTIs and unilateral or bilateral VUR underwent endoscopic injection of Macroplastique. Several months after the procedure, they developed flank pain, high-grade fever, and oliguria, and were diagnosed with ureteral obstruction, urosepsis, acute renal failure, or VUR. Intravenous antibiotics were administered and percutaneous nephrostomy was performed. However, unfortunately, all the patients had to ultimately undergo ureteroneocystostomy [1].
Recently in Korea, a small number of case reports similar to ours have been published. In one study, a 10-year-old girl, underwent subureteral administration of Macroplastique to treat bilateral VUR, following which she had recurrent pyelonephritis. US revealed two bladder stones (2.0 cm and 1.3 cm) near the right trigonal area of the bladder, 6 years after the endoscopic injection. Complete stone removal using cystolitholapaxy was performed [10]. In another study, a 38-year-old male patient who had undergone Macroplastique injection 7 years ago due to VUR, had left sided abdominal pain. CT abdomen showed a stone (0.83 cm) near the left UVJ and it was removed using Holmium laser. As seen in our case report, both patients who were injected with Macroplastique several years ago had stones in the bladder or at the UVJ. After removing the stones with laser treatment, recurrent pyelonephritis and abdominal pain disappeared completely [11].
Calcified Macroplastique substance in the submucosa can lead to mucosal erosions as it is grows. If mucosal erosions get worse, hematuria and symptoms of cystitis may develop, which if untreated, may lead to UVJ obstruction. Considering the increasing number of patients of VUR receiving Macroplastique injection, long term standardized follow-up is required, and physicians should recognize the late complications after endoscopic bulking agent administration. Also, recurrent hematuria after endoscopic injection should be thoroughly evaluated.
Notes
Ethics statement
This study was approved by Pusan National University Yangsan hospital's Institutional Review Board (IRB No. 05-2018-136).
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.