


Introduction
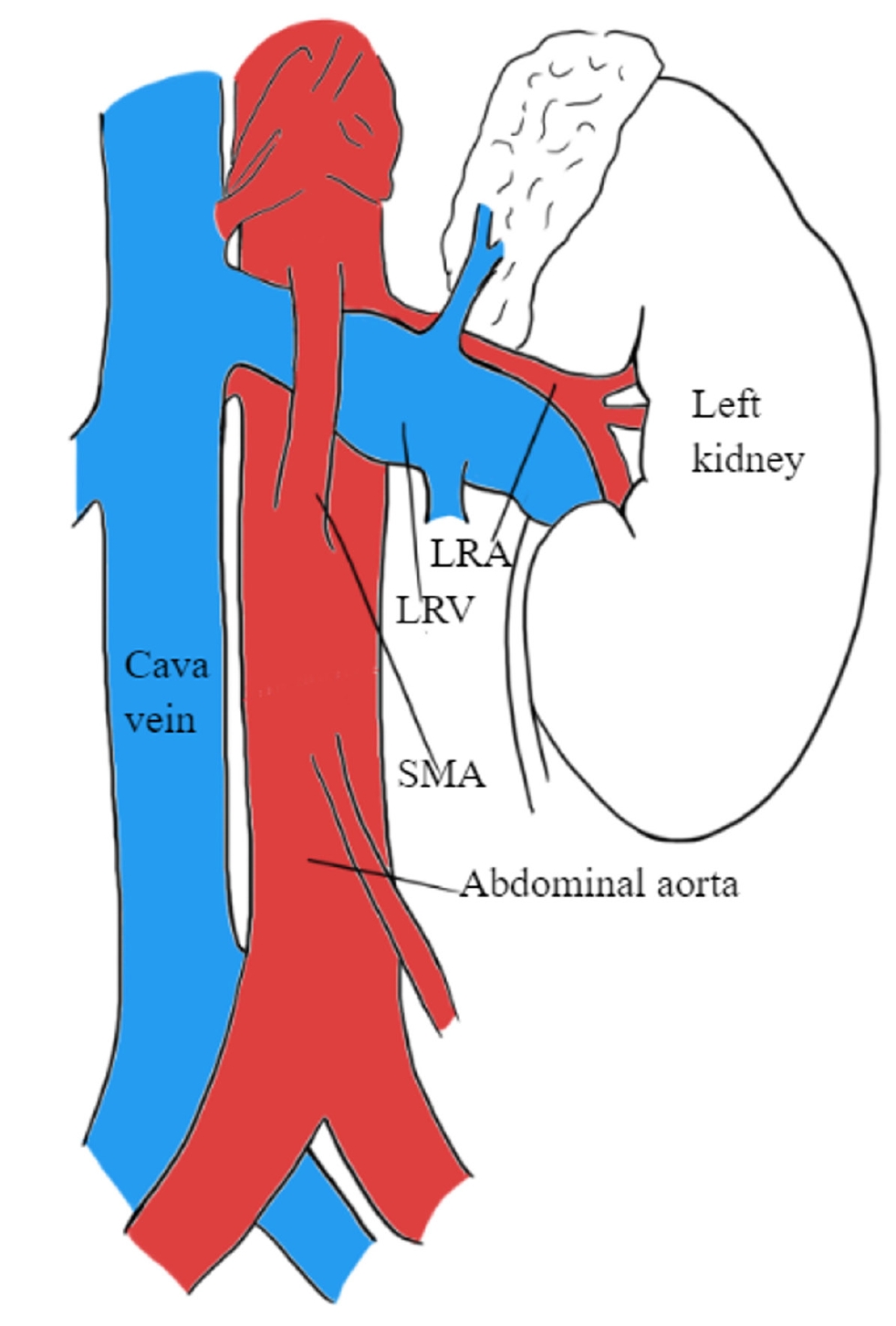
Renal nutcracker syndrome (NCS) is a rare pediatric disease that is defined as the symptomatic entrapment of the left renal vein (LRV). In the anterior form, the LRV is compressed between the aorta and mesenteric artery (Fig. 1), or less commonly between the aorta and vertebral column, known as posterior NCS. Common symptoms include hematuria, proteinuria, and flank pain, known as ŌĆ£TriadeŌĆÖs symptoms,ŌĆØ although there is still wide variability in clinical presentation among children [1-3]. Symptoms are believed to result from increased pressure within the renal vein and the kidneyŌĆÖs venous drainage system. This elevated pressure is believed to harm the thin-walled septa between the veins and the collecting system in the renal fornix, leading to hematuria or proteinuria [2]. However, pathological evidence supporting this hypothesis is still lacking [4].
Although the terms ŌĆ£nutcracker phenomenon (NCP)ŌĆØ and ŌĆ£NCSŌĆØ were used interchangeably in earlier literature, NCP specifically refers to the anatomical structure without the occurrence of symptoms [1,4,5]. The first pathological description of this anatomical structure was attributed to the anatomist Grant in 1937 [1], following the first clinical report of the phenomenon by El-Sadr and Mina in 1950 [6]. The term ŌĆ£NCSŌĆØ is commonly attributed to the Belgian physician de Schepper [7], although it was initially used by Chait et al. in 1971 [8].
While there is extensive research on NCS in adults [2,4], the incidence, diagnostic criteria, and treatment remain undefined in the pediatric cohort due to its rarity in children [9]. The exact incidence of NCS in children remains unknown [4]; however, a peak age period of diagnosis was observed between ages 10 and 14 years [10,11]. Timely identification of NCS is crucial due to the potential occurrence of more severe complications such as severe anemia or renal vein thrombosis resulting from hematuria [12]. Given the wide variability of NCS in the pediatric population, this literature review aimed to provide a better comprehensive understanding and overview of the disease in children.
Symptoms and clinical features
A wide range of symptoms has been observed in children with NCS due to the varying hemodynamic consequences of LRV compression [13]. LRV compression raises the retrograde venous pressure, impacting other associated vessels and leading to various clinical manifestations [14].
The most common symptoms observed in children with NCS are hematuria (micro- and macrohematuria), proteinuria (mainly orthostatic), and flank pain [3,5,9,13,15]. Additional studies observed symptoms such as renovascular hypertension, unspecified abdominal pain, dysmenorrhea, nephrolithiasis, calciuria, fatigue, testicular or scrotal pain, and varicocele [3,11,16,17]. Symptoms also often worsen with physical exercise [2,3].
Hematuria is the most frequently observed symptom in pediatric patients [3,7,18], occurring due to increased venous pressure leading to varicose veins rupturing and consequently bleeding into the renal collecting system [9,16]. Hematuria has been reported as the most frequent symptom in 75% of pediatric patients with NCS [3]. Children often experience microscopic hematuria asymptomatically, compared to adults, who more often experience hematuria with pain [11]. Additionally, a systematic review on pediatric NCS analyzing published literature from 1990 to 2020 described hematuria as the most commonly experienced symptom, observed in approximately 55% of children with NCS. This was followed by proteinuria and flank pain, observed in approximately 50% and 19% of children, respectively [9].
Although NCS can develop in individuals of all age groups, a higher incidence is observed in underweight or lean children aged 10 to 14 years, with a slight prevalence among females [14]. In a systematic review assessing 423 children with NCS (218 males and 205 females), the mean age of the study participants was 12 years [9].
Diagnosis and diagnostic criteria
Due to the rarity of NCS in children and a limited number of published studies, standardized diagnostic criteria for NCS in pediatric patients are lacking. Diagnosis often relies on exclusion criteria and utilizes conservative and invasive techniques [19].
In adults, renal venography is the first-line diagnostic examination [20,21]; other standard diagnostic techniques include renal Doppler ultrasonography (USG), magnetic resonance angiography, computed tomography (CT), and multislice helical CT angiography [22-25]. In contrast, many noninvasive diagnostic techniques, such as Doppler USG, magnetic resonance imaging (MRI), or CT, are initially recommended for children [26-28]. As varicocele is often observed simultaneously with NCS in approximately 33% of male pediatric patients, Doppler USG is further recognized as an effective diagnostic technique [3]. Additionally, urinalysis helps identify potential NCS manifestations, including repeated hematuria (gross or microscopic), calciuria, and orthostatic proteinuria [9,29].
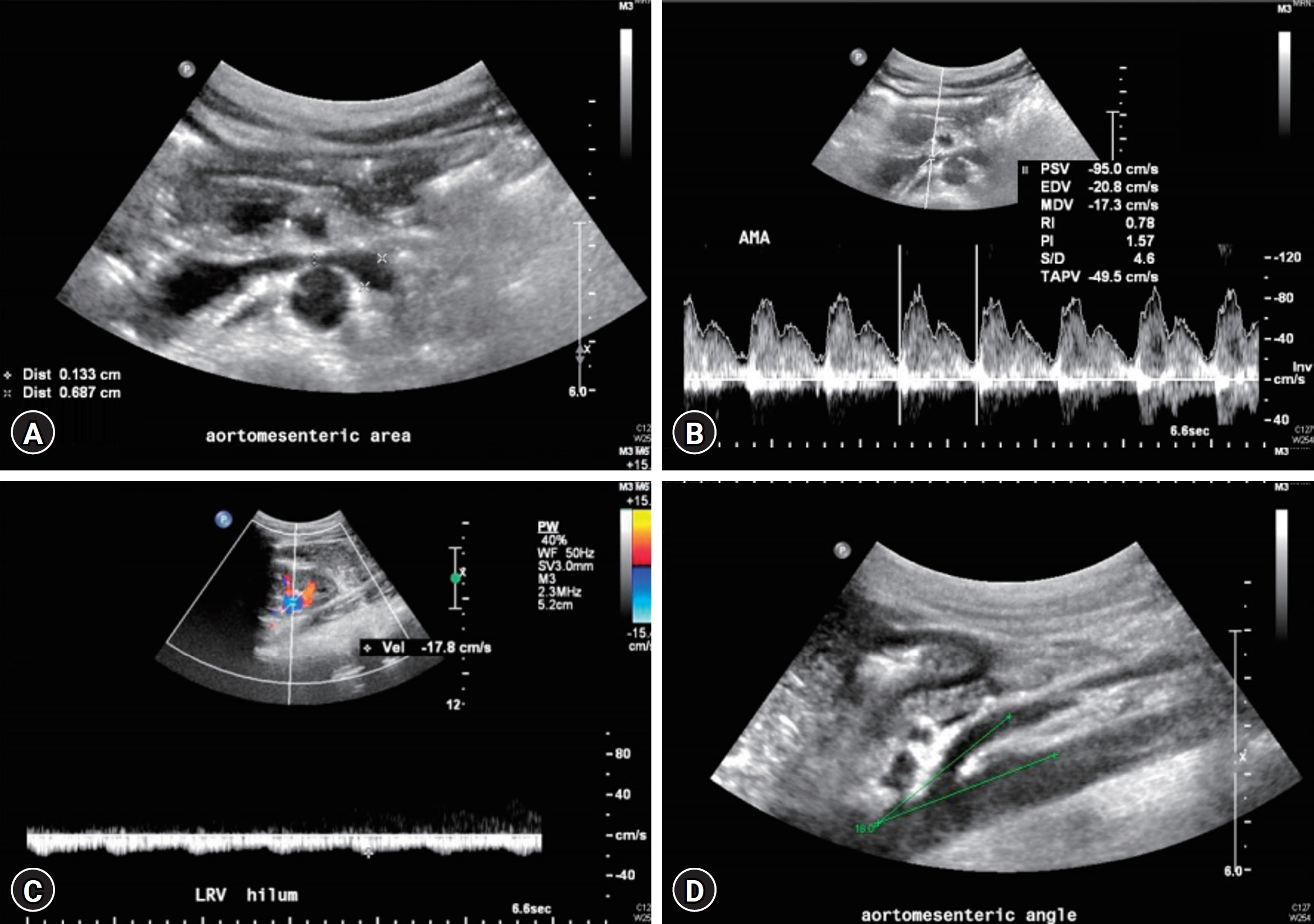
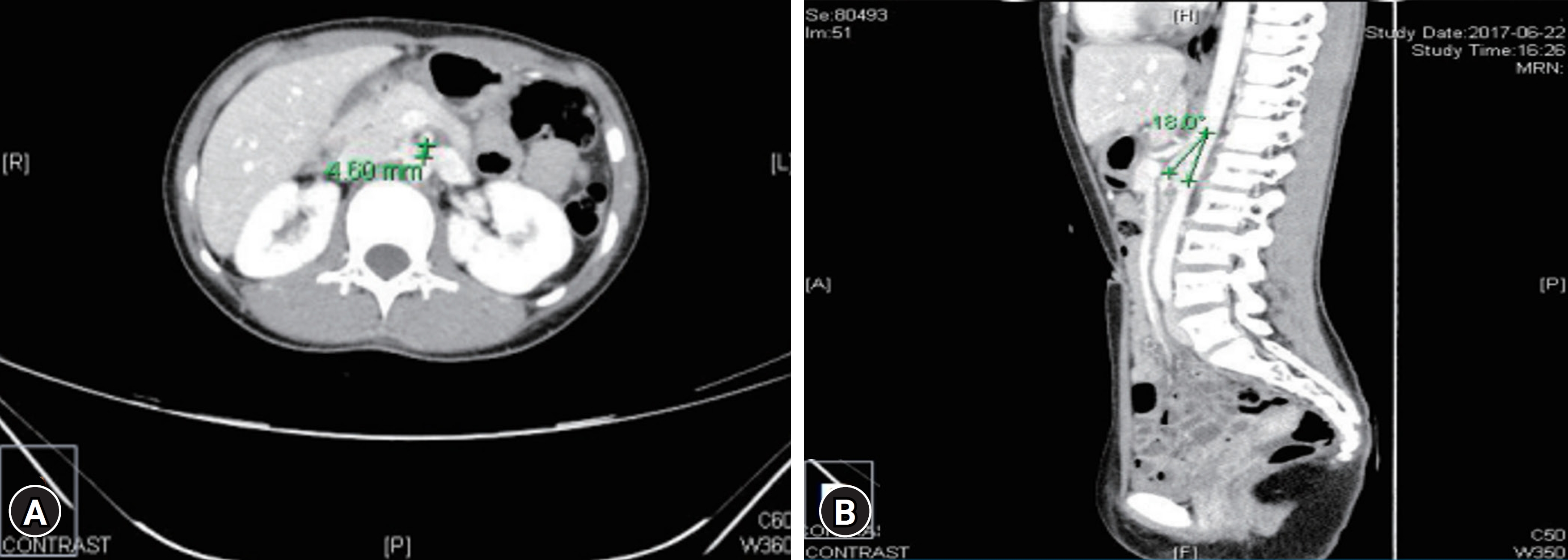
In children, recommended noninvasive examinations such as abdominal USG and Doppler studies are reported to have a sensitivity and specificity of approximately 82.3% and 89%ŌĆō100%, respectively [3]. In the general population of patients with NCS, an aortomesenteric (AOM) angle of <35┬░ is significantly characteristic of diagnosis (Figs. 2, 3) [30]. A previous study involving 205 pediatric patients reported an AOM angle of <25┬░ in approximately 9% of asymptomatic pediatric patients with NCS [31]. Additionally, a study including 39 pediatric patients with orthostatic proteinuria reported that a ratio greater than 0.6 between the AOM angle in the upright and supine positions could be diagnostic of NCS [32]. However, additional criteria and further studies are required to validate the exact cutoff angle [20,33].
The diameter of LRV and peak velocity ratio in the AOM and hilar portions can also serve as diagnostic criteria for NCS in children (Figs. 2, 3) [3,9]. According to a study in 2002, a ratio greater than 4.2 for the diameter of LRV and 4.0 for the peak velocity ratio can be used as cutoff values to diagnose NCS [22]. A study enrolling a group of 12 pediatric patients published in 2006 recommended a peak velocity cutoff value of 4.7 (with specificity of 90% and sensitivity of 100%) [23]. Consequently, a study in 2007 including 216 pediatric patients with isolated hematuria that reported NCS in approximately 33% of patients recommended a peak velocity ratio of at least 4.1 [24]. These varying results highlight the need for further research to validate peak velocity or LRV ratio cutoff values in diagnosing NCS.
Although conservative techniques are often recommended for diagnosis, invasive diagnostic techniques such as intravascular USG or phlebography are performed under circumstantial cases to assess the obstruction severity [9,28,29]. These invasive techniques may involve catheterization to measure the pressure gradient between the inferior vena cava (IVC) and LRV. The typical pressure gradient between IVC and LRV in the general population is <1 mmHg [28]. When the pressure gradient exceeds 3 mmHg, a definitive diagnosis of NCS is established [21,25,28]. Renal biopsies, venography, arteriography, cystoscopy, and intravenous urography are additional invasive techniques used in children [9].
Comorbidities and complications
Comorbidities frequently observed in pediatric patients with NCS include varicocele, chronic fatigue syndrome or idiopathic chronic fatigue, superior mesenteric artery (SMA) syndrome, and WilkieŌĆÖs syndrome [34-39]. Table 1 describes the comorbidities observed in pediatric patients with NCS from previously published studies.
Varicocele is characterized by the enlargement of veins within the scrotum and exhibits a direct association with NCS in male children [34]. In cases where NCS is present, it can contribute to the development or exacerbation of varicocele [40]. A study involving 3,042 patients with varicocele, including 858 LRV entrapment cases, reported a risk ratio of 43.3 for LRV entrapment-associated varicocele recurrence [34].
Furthermore, occasional associations have been observed between chronic fatigue syndrome and NCS, characterized by elevated LRV-IVC pressure gradients. Fatigue symptoms have shown a positive correlation with high peak velocity ratios through Doppler USG; in some instances, these symptoms have improved postoperatively [41-43]. This association was also reported in a study that observed nine pediatric patients with severe NCP and chronic fatigue syndrome or chronic fatigue [35]. Additionally, two case studies have reported the coexistence of NCS with SMA syndrome in a 15-year-old male and a 14-year-old female [36,37]. WilkieŌĆÖs syndrome has also been recorded to occur concurrently with NCS in two case studies with 15-year-old and 17-year-old males [38,39].
Additional complications unrelated to NCS but observed in pediatric patients with NCS include immunoglobulin A nephropathy, immunoglobulin M nephropathy, intussusception, Henoch-Sch├Čnlein purpura, right retrocaval ureter, urolithiasis, LRV duplication, renal abscess, midline congestion syndrome, celiacomesenteric trunk anomaly, intestinal malrotation, and spontaneous spermatic vein thrombosis [44-55].
Treatment
Two main treatment approaches for NCS include conservative and surgical treatments. In adults, surgical treatment is often considered the initial therapy of choice. Conversely, in pediatric patients, a conservative approach, often involving a watch-and-wait strategy, is typically recommended for a minimum duration of 2 years [40,56,57]. The choice between conservative and nonconservative management is controversial and often depends on the clinical status and severity of symptoms [58].
The recommendation for conservative management in children is supported by previous studies that have demonstrated the spontaneous resolution of symptoms as children undergo physical development. According to a comprehensive systematic review, out of 138 pediatric patients who received conservative treatment for NCS, approximately 95% achieved complete resolution or symptom improvement (43% or 52%, respectively) [9]. Regarding hematuria in pediatric patients with NCS, after a mean follow-up of 1.5 years, 75% of pediatric patients experienced a complete resolution of hematuria. This study also recorded a significant increase in patient height and weight and a significant decrease in LRV and peak velocity ratios, suggesting how body mass index (BMI) may be a potential hemodynamic factor for the spontaneous resolution of hematuria [59].
Although the exact mechanism behind the spontaneous resolution of symptoms remains unclear, adolescent growth and an increase in BMI may be indicators for the prognosis of NCS. A study involving 23 children with NCS showed a significant correlation between BMI and the regression of hematuria and proteinuria symptoms. The study reported an initial average BMI of 16.9 kg/m2, significantly increasing to 18.6 kg/m2 during the follow-up period [16]. An increase in body weight in adolescents often modifies the position of the left kidney, allowing for a decrease in pressure on the LRV [4,16]. Additionally, the physical growth of the patient can prompt fibrous tissue proliferation at the origin of the SMA, partially relieving the compression at the AOM angle [40].
Although conservative treatment is highly recommended, when severe NCS symptoms persist, various surgical and endovascular treatments techniques may be applied. Common surgical treatments include the LRV, SMA, or left gonadal vein transposition, kidney autotransplantation, endovascular stent placement, laparoscopy, and shunt operation [60-65]. Among them, LRV transposition is considered the gold standard surgical treatment for uncompensated NCS. Other surgical options depend on the patientŌĆÖs specific case and context, such as symptoms severity, stage of the syndrome, and patient age [9,66]. For example, in a cohort of 53 male pediatric patients diagnosed with NCS and varicocele, spermatic-inferior epigastric vein anastomosis was performed. Approximately 96% and 49% of patients experienced improved NCS and scrotal bulge symptoms postoperatively [67]. Another example of case-specific operative treatment was recorded in managing NCS in a 16-year-old female. In situ, gonadal vein valvotomy and side-to-side gonado-iliac bypass were performed, resulting in a complete resolution in the patient [68]. Furthermore, in a case study of a 14-year-old female with NCS, orthostatic proteinuria resolved after angiotensin-converting enzyme inhibition therapy, although this treatment may affect renal hemodynamics in children [15,69].
In summary, NCS treatment varies depending on the patientŌĆÖs specific context. However, further clinical studies with long-term follow-up are required to evaluate the effectiveness of different treatment approaches.
Conclusions
Early diagnosis of NCS is crucial to prevent severe complications such as anemia or renal vein thrombosis. NCS symptoms vary widely, including hematuria, proteinuria, and flank pain. Due to pediatric NCSŌĆÖs rarity, diagnostic criteria are not well-established, although common noninvasive diagnostic techniques include Doppler USG, MRI, and CT for initial diagnosis. Comorbidities associated with NCS in pediatric patients include chronic fatigue syndrome, chronic fatigue, varicocele, SMA syndrome, and WilkieŌĆÖs syndrome. Treatment options for NCS range from conservative management to surgical interventions. Further research and clinical studies with long-term follow-up are necessary to establish standardized diagnostic criteria and evaluate the efficacy of different treatment approaches for NCS in pediatric patients. These studies should additionally focus on evaluating the accuracy of noninvasive techniques, exploring the impact of associated comorbidities, and assessing the efficacy and safety of different treatment approaches. A better understanding of NCS in children will enable early management and improved outcomes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




